
Dermatome Map
How was this made?

Hey there,
Are you one of the people who is fascinated by how things were developed? Have you ever thought about how dermatome maps were developed and what experiments were performed to create dermatome maps? This time I will write about the two dermatome maps that were developed and are still in use nowadays.
What is Dermatome?
The word ‘Dermatome’ is combined with two Greek words ‘derma’ and ‘tome’, which is the skin for ‘derma’ and the thin segment for ‘tome’. The dermatome is an area of skin innervated by the dorsal root of a single spinal nerve. As these roots are arranged in segments, that’s why it is referred to as thin segments of skin.
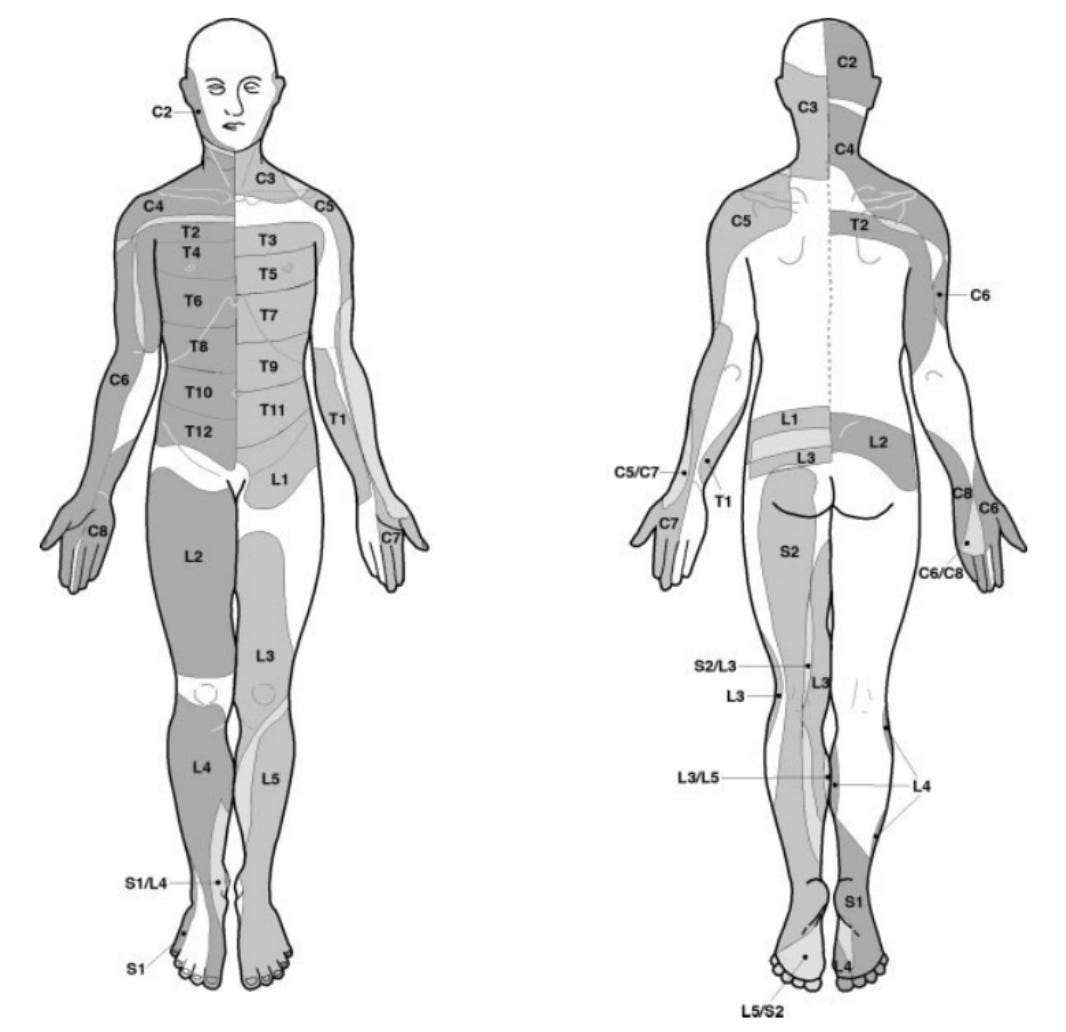
Foerster map (1933)
Foerster conducted clinical observation to examine patients with sensory disturbances, trying to find out the pattern of sensory loss. As Foerster is a neurosurgeon, he isolated a single dorsal nerve root by surgical section of at least two adjacent dorsal nerve roots both above and below and mapped the residual area of cutaneous sensation in humans. At least two patients were used as case studies to identify each level of dermatome (C2-S2), therefore the ethics of this study are questionable.
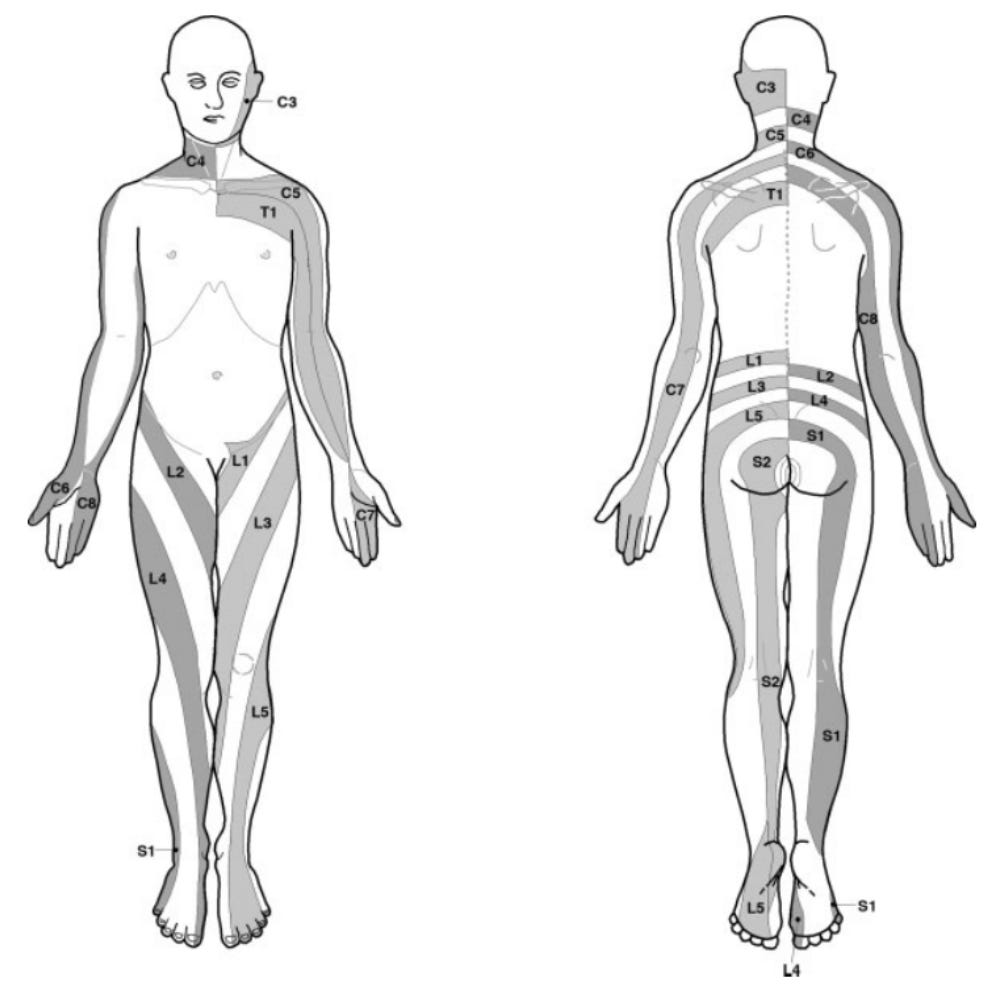
Keegan and Garrett map (1948)
Keegan and Garett aimed to extend Foerster’s observation by using other methods, however, thoracic dermatomes were not studied at all. They recruited a large number of patients with disc-prolapsed and performed both surgical and non-surgical case studies on patients. They performed light pin scratches (non-surgical) to identify patients with hypoalgesia and were also aware of the distribution of radiating pain. They realized the areas of hypoalgesia were different from the map that Foerster created, so further studies were made to develop the ‘new map’. Surgeries were performed to confirm and verify the compression of a single nerve root within a large number of patients.
As a prolapsed disc could affect more than one root, Keegan and Garrett note that some cases of hyposensitivity were only found at the distal part of the limb, but they did not further discuss or comment on it.
Hopefully, this newsletter further expands your understanding of dermatome mapping. What are your thoughts and feelings about the dermatome map that we are using? Feel free to comment or DM me through @talk.physiotherapy !